Emergency Medicine Teaching Case: A Case of Compartment Syndrome
Forty year-old male with a history of polysubstance abuse presented to the ED c/o intense pain and swelling of his right lower extremity (RLE) for the past two days. Patient used heroin two consecutive nights prior to presentation and reports falling asleep with his RLE folded underneath his body.
When he woke up in the morning, the leg was swollen and painful to touch. Patient states he could not move his leg due to severe pain. As the day progressed, patient noticed increasing pain and swelling of the leg in addition to the leg turning a blueish color. Patient then presented to the ED.
Upon arrival in the ED, pt was hypotensive, tachycardic, c/o severe pain in RLE.
On PE, the RLE below the knee was severely tender to touch and the soft tissue was very tense. RLE appearance is below.
Click to View RLE Appearance (graphic image)
Labs:
- WBC- 18.4
- Hgb- 8.0
- Na- 133
- K- 6.2
- Ca- 6.0
- Cr- 6.4
- GFR- 10
- Lactic Acid- 3.8
- CK- 188
With this history, compartment syndrome was strongly suspected. Compartment pressures were measured with a Stryker Device. Compartment pressures of the RLE were as follows:
Anterior compartment = 19 mm Hg
Lateral compartment = 16 mm Hg
Posterior compartment = 4 mm Hg
IVF resuscitation and broad-spectrum IV antibiotics were initiated. Surgery was consulted and pt was taken to the OR emergently.
Compartment Syndrome
Consider compartment syndrome after: fracture (most common), crush injury, immobilization, snake bites, burns, prolonged tourniquet application, fluid extravasation into a limb, soft tissue infection, and extreme exertion.
Immediate threats: nerve and muscle viability
Later threats: infection, gangrene, rhabdomyolysis, renal failure
Clinical symptoms:
– Compartment is swollen, firm, tender
– Usually apparent after trauma/injury, but may be delayed up to 48 hrs after the event
– 5Ps: Pain (early), Paresthesia (early), Pallor, Paralysis(late), Pulselessness(late)
Leg Compartments:
Workup:
– X-ray to evaluate for fracture
– Compartment pressure measurements (commercially available Stryker Device)
· Normal is <10 mm Hg
· Delta Pressure: ΔPressure = Diastolic BP – Compartment pressure (ΔPressure<30 mm Hg is suggestive of Compartment Syndrome)
– Total CK to evaluate for rhabdomyolysis
– Chemistry for hyperkalemia/renal failure
Management:
– ABC
– IVF fluid resuscitation
– Abx
– Analgesia
– Supportive treatment (rhabdomyolysis, renal failure, hyperK, etc)
– Emergent OR for fasciotomy
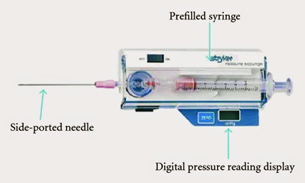
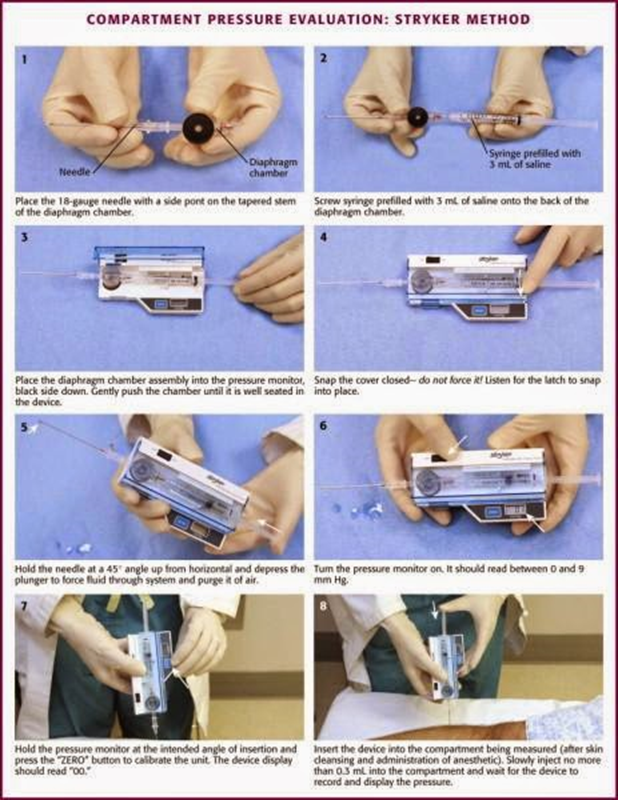
Stryker Device
The Stryker Device is a type of hand-held manometer which performs direct measurements of compartment pressures.
Compartment pressure measurement with Stryker device. This is a great diagram from emcurious.com blog.
References:
1. Wiki EM “Compartment Syndrome”
2. http://www.emcurious.com/blog-1/2014/12/11/compartment-pressure-measurement-stryker-it
Courtesy of:
Syed Wajid Ali, MD
EM resident class of 2021
Karima Sajadi, MD
Associate Residency Program Director
Crozer Chester Emergency Medicine Residency
Upland, PA
Contact Information
Karima Sajadi-Ernazarova, MD
Associate Professor of Emergency Medicine
215.762.2374 | karimasajadi@gmail.com
The information on these pages is provided for general information only and should not be used for diagnosis or treatment, or as a substitute for consultation with a physician or health care professional. If you have specific questions or concerns about your health, you should consult your health care professional.
The images being used are for illustrative purposes only; any person depicted is a model.
Back to Top