Why do we need to monitor adolescent tobacco control policies in cities?
An analysis of the historical Global Youth Tobacco Survey datasets
Posted on
January 28, 2021
By: Sharon Sanchez-Franco, Carolina Pérez-Ferrer, Amy H. Auchincloss, Francisco-Javier Prado-Galbarro, and Tonatiuh Barrientos-Gutierrez
SALURBAL Project
Tobacco use is the main preventable cause of chronic diseases and premature death around the world. Preventing tobacco use during adolescence is critical, because smoking initiation is most common during that life stage. Also, adolescents are highly susceptible to social influence, a characteristic that is known and exploited by tobacco companies.
The World Health Organization (WHO) has been leading the global efforts to reduce tobacco use in the world, through the Framework Convention on Tobacco Control (FCTC). To date, 12 countries in Latin America have ratified the FCTC. Advances in tobacco control in the region have been heterogeneous across countries, as has been documented by WHO.
Latin America is one of the most unequal regions in the world. The gaps in wealth, income, and education within countries are staggering. Tobacco control efforts and results in the region could also be heterogeneous across cities, reflecting different levels of development, implementation, surveillance and enforcement. In the paper entitled “Adolescent tobacco exposure in 31 Latin American cities” we analyzed tobacco control policies and tobacco use as reported by 132,065 adolescents from six countries (Argentina, Brazil, Chile, Colombia, Mexico, and Peru) to identify the progress before and after the FCTC.
To monitor the control tobacco policies at the country and the cities level, we made a conceptual proposal based on the MPOWER package, which is used by the WHO to track the status of the tobacco epidemic. The following table shows the six MPOWER domains and the indicators we used from the Global Youth Tobacco Survey (GYTS) and WHO reports.
| Domain of control tobacco policies |
WHO policy implementation report [1]
|
Adolescent report in the GYTS [2] |
| Monitor tobacco use and prevention policies |
Prevalence of tobacco use and estimated trend* |
Students who use tobacco products |
Protect people from tobacco smoke
|
National smoking bans and enforcement |
Student exposed to smokers at home and in other
places
|
| Offer help to quit tobacco use |
Cessation services are available, and costs are covered |
Smoker students have received help or advice to
help them stop smoking* |
Warn about the dangers of tobacco
|
Law mandates health warnings on tobacco packages |
Anti-tobacco education in school |
Enforce bans on tobacco advertising, promotion,
and sponsorship |
Bans on advertising, bans on discounts,
product placement
|
Retailers refuse to sell cigarettes to minors.
Media and advertising.
Offers for free cigarettes |
| Raise taxes on tobacco |
Tax as a share of the retail price, and affordability
|
The cost of cigarettes is related to access and
availability of tobacco products for students* |
[1]Collected from reposts of the World Health Organization. [2]Collected from Global Youth Tobacco Survey. *These indicators were not included in the study.
A very important result in the region is the data availability across countries and cities. Just six countries (Argentina, Brazil, Chile, Colombia, Mexico, and Peru) had data from the GYTS to compare pre and post-FCTC periods. From them, just Brazil, Mexico, and Peru included data from two or more cities. The lack of information across the region shows that cities should be more committed to monitoring permanently and frequently the tobacco epidemic using standardized surveys.
A Heterogeneous Region
According to WHO, tobacco control policies improved in the post-FCTC period in the entire region. Chile and Brazil were rated excellent, Colombia and Argentina had the largest improvements, while Peru and Mexico had the lowest scores. However, when analyzing the GYTS data, advances within countries were highly heterogeneous, with some cities making stronger improvements than others. We observed overall improvements in tobacco use, protection against tobacco smoke at home, and tobacco education, while exposure to media and advertising didn’t change.
To illustrate the differences of advances in tobacco control within and between countries, we show in Figure 1 the prevalence of adolescent use of tobacco for 30 days in Argentina, Brazil, Chile, Colombia, Mexico, and Peru (see Figure 1). Most countries had decreases in the prevalence of adolescent smoking; however, there are large differences across the region and within countries in the tobacco use prevalence and change pre and post ratification.
For example, across the region, the pre-ratification adolescent tobacco use prevalence varies from 15.5% in Culiacan (Mexico) to 38.4% in Santiago (Chile). By post ratification FCTC period, Culiacan had a favorable decreased of 33% of their prevalence; meanwhile, Santiago decreased the 7% of their prevalence. Large differences are also across the cities within countries. For instance, within Brazil, after ratification FCTC, the prevalence in Curitiba increased by 12% and Fortaleza decreased by 28%. These results show that even with the same national policies, the implementation at the city level varies widely.
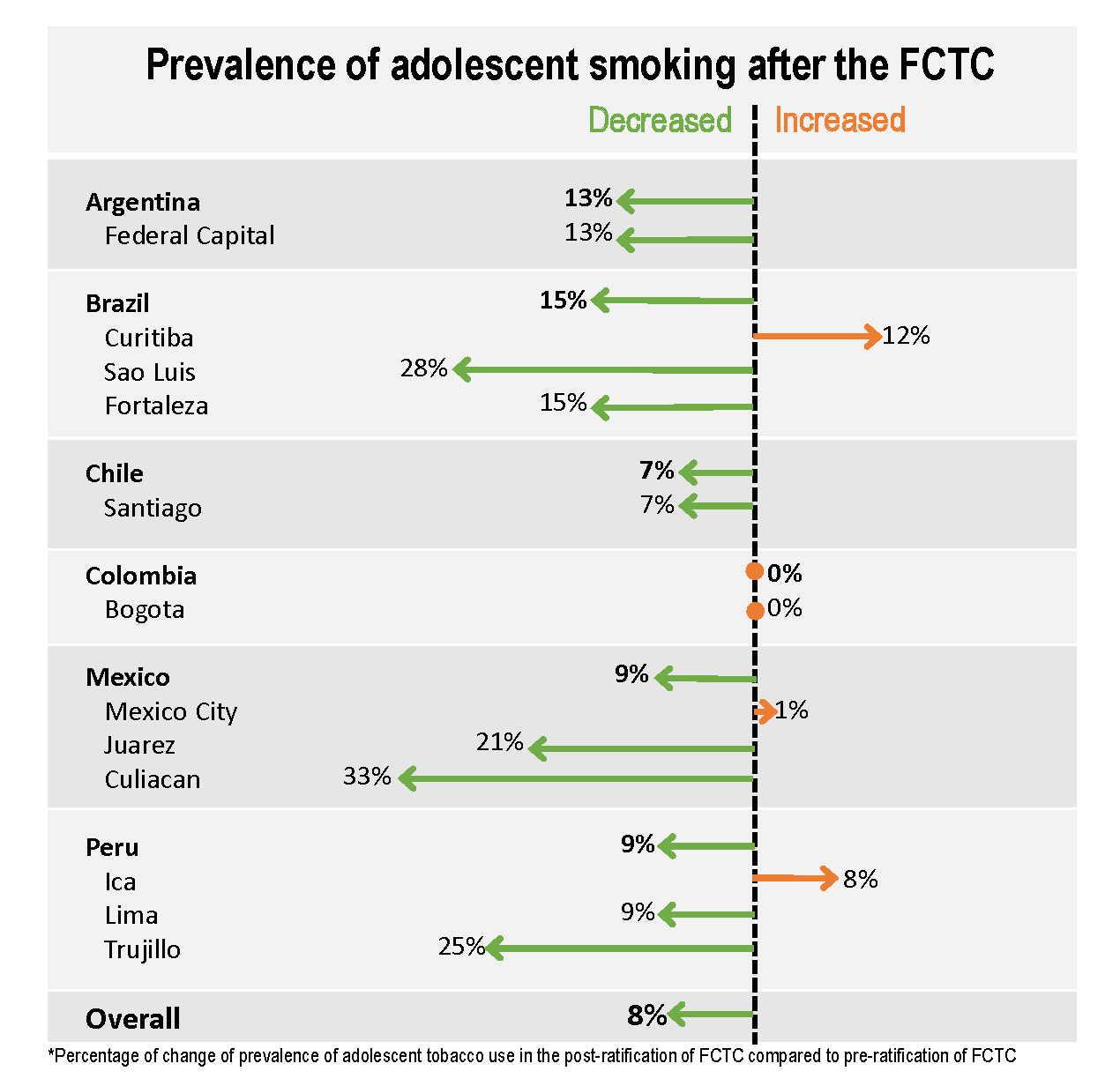
Figure 1.Monitor tobacco use indicator from GYTS: Prevalence of adolescent use of tobacco in past 30 days and prevalence ratio of pre : post-FCTC period by country and by city.
Other indicators of MPOWER are also important and also heterogeneous. For example, school-based programs are important to increase the knowledge about tobacco risks but also to develop personal skills to refuse tobacco products. Thus, this indicator is useful to assess policies that warn against the dangers of tobacco, but also reflects the ability of countries and cities to articulate different sectors, such as education and public health.
We found that Brazil and Colombia decreased anti-tobacco education in school reported by students after the FCTC. Meanwhile, Argentina, Chile, and most cities of Mexico and Peru increased anti-tobacco education in schools. We observed large heterogeneity across cities in this indicator. For example, within Mexico, Tijuana had a very strong increase in anti-tobacco education in schools, while Guadalajara almost had no change. Similar differences can be observed in countries that had information at the city level, such as Peru and Brazil.
The large within-country heterogeneity in prevalence and change for most indicators is an important finding. It suggests that we need to reconsider the relevance of cities as key areas to monitor tobacco control policies and the changes in the pandemic in the region. In addition, it reflects a paradigm of tobacco control monitoring that assumes that the most relevant level of monitoring is the country-level, and that capital cities are an adequate proxy for national estimates, which is clearly not the case.
Monitoring at the country-level or only in capital cities could be hiding large inequalities within countries; this could severely limit tobacco control policy advances. Our findings show that even with the same national laws, some cities have much better implementation results than others. Cities could learn from other cities in governance and commitment to preventing tobacco use among adolescents in the local context. Further efforts are needed to increase the granularity of tobacco surveillance to reach the city level. Also, efforts at the city level are needed to secure the correct implementation of tobacco control recommendations.
To read the full article, published on October 12, 2020, click here.