July 24, 2019 Emergency Medicine Conference Recap by Dr. Karima Sajadi
8:00 am Case conference by Dr. Alin Gragossian
Intern in "hot seat": Dr. Mike Ambrose
Senior "Lifeline": Dr. Jon Skilton
CC: Nausea/abdominal pain
Mesenteric ischemia
Risk:
A/fib and other dysrhythmias
Hypercoagulable state
Endocarditis
CHF
CKD
CAD
SMA most commonly affected artery, most commonly from embolization from heart
Usually arterial occlusion, but can be venous or NOMI
Presentation:
Abd pain, especially post-prandial
GI bleeding
Diarrhea
N/V
Anorexia
Hypotension
Tachycardia
Dx workup:
Mesenteric angiography is gold standard
CT angiography – most commonly used (triple-phase is preferred)
Lactate/d-dimer – may be helpful
Treatment:
NPO
IVF resus
Pain control
Abx for perforation prophylaxis
Early surgical consult, need to go to OR asap
IR can be indicated
Complications:
Sepsis
Perforation
Necrosis
Death
9:00 am Resident lecture competition
"What are people afraid of?" by Dr. Mathew St. Marie
Orchidiophobia – fear of snakes and spiders
Snakes: 5000 native snake bites in USA annually
25% are dry (no envenomation)
Cytotoxic – rattlesnakes, copperheads
Causes local tissue injury, DIC
Most damaging
Can cause compartment syndrome
Neurotoxic – coral snakes
Respiratory paralysis with minimal local tissue damage
Most deadly
Presentation:
Story consistent with bite
May or may not see the bite
Fang marks, localized pain
Progressive edema/ecchymosis
N/V, dizziness, muscle fasciculations
Hypovolemic shock
Evaluation:
CBC
CMP
Coags
Fibrinogen
Look for local injury, compartment syndrome, expanding ecchymosis – mark the site
Management:
Remove jewelry
Immobilize the limb
Measure circumference
Antivenom
Dry bite: dispo after 6 hrs
If antivenom – admit to ICU
"Tetanus" by Dr. Cortnie Carlheim
Low incidence in USA due to vaccination
Mortality 20-30%
Age >65 yo
Contracted from puncture, contaminated
Causes painful muscle contractions
10:00 am "Neonatology in a Nutshell" by Dr. Yanick Vibert
When you receive a call about newborn arriving, do:
1. Turn the baby warmer ON –
Heat loss:
Conduction – from the back of the baby where baby is lying on the warmer, so turn it on asap
Convection - around the baby, so put sides up on the baby warmer
Evaporation - from baby is wet, do dry it up from head down, then put the hat on
Radiation – from cold objects around (cold walls, temp of the room, etc will draw heat from baby)
Turn from manual mode to baby mode when the baby is placed on the warmer and the probe is attached to the baby
When baby is hypothermic, there is a risk of hypoglycemia
During normal labor, baby looses all the fluid from the lungs while passing through vaginal canal and they get filled up with air. If baby is a C-section, then all that fluid is in the lungs: tachypnea, resp distress, etc.
2. Suction – bulb vs catheter
Bulb: squeeze first, do sideways into mouth, let the bulb go so it will suck the secretions, then take it out and shake it out. Do not put the beek straight into the mouth because it will invoke vagal response. Then do nostrils.
Catheter: gastric secretions as well. Keep pushing catheter into stomach, while suctioning, don’t stop a the throat to prevent vasovagal response.
If you suspect choanal atresia, baby will be blue/cyanotic, but will pink up when crying. It’s because babies are obligate nose breathers, and crying makes them breath through mouth.
Introduce all members of resus team
HOB: airway
Right side: pulse ox/vitals
Left side: Neonathology
Preductal vs post-ductal saturation: "I pledge allegiance to ductus" – everything above the right arm is pre-ductal.
Glucose: 40-50 wnl, < 40 is hypoglycemia
D10: 2ml/kg bolus, then 80ml/kg/day drip (with Ca for heart muscle)
Correct size of mask for BVM: mask needs to cover both nose and mouth
Term baby is 38 weeks
41-42 weeks is post-term
< 36 weeks is preterm
If baby is crying, HR is >100
Umbilical artery pulse: if squeeze at the point of the belly, you will feel "stampeding horse"(>100) vs "slow walk in the park"
Look at PMI as well.
Auscultate with stethoscope.
Apnea – no breathing for 20 sec
Primary apnea – in-utero, dry up and stimulate the baby, it should go away
Secondary apnea – stimulating does not do it, need NIPPV
Hyperextend the head back, roll the mas from nose to mouth, position correctly, get a nice seal and start bagging. Do not press down the mask onto baby’s face, because you will block the airway. Bag just enough to see until chest wall is rising.
Resp rate: every "Mississipi"
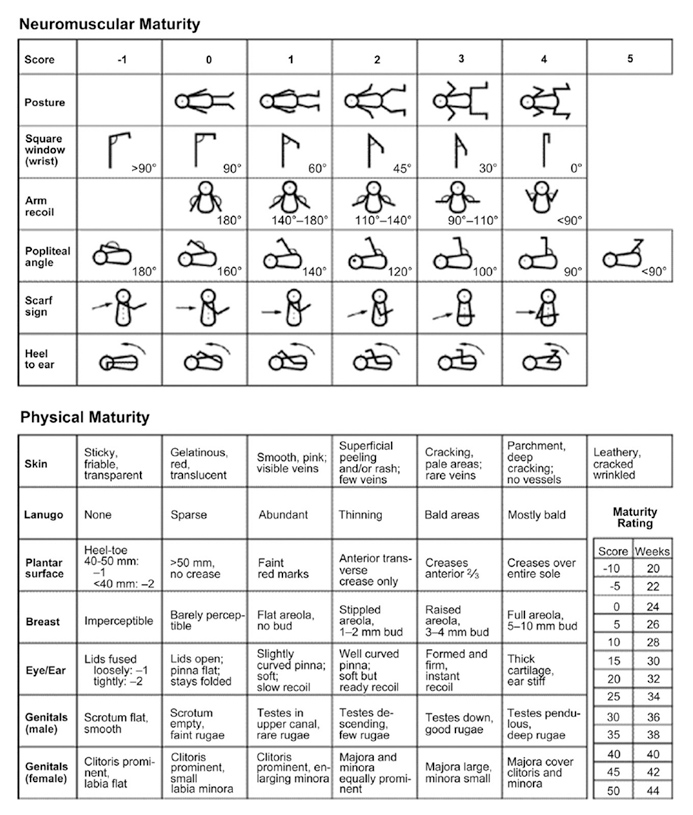
Estimating gestational age:
24 week – straight, no flexion
24-25 weeks increased flexion at ankle
26-27 flexion at wrist
28-30 – knees
30-31 – elbows
32-33 – hip
36-38 – shoulder girdle, able to lift/move shoulders and bring arm to opposite sholder at a sharper angle
Ballard score:
The information on these pages is provided for general information only and should not be used for diagnosis or treatment, or as a substitute for consultation with a physician or health care professional. If you have specific questions or concerns about your health, you should consult your health care professional.
The images being used are for illustrative purposes only; any person depicted is a model.
Back to Top